|
|
|
Recipe for National Insolvency (June 9, 2008) You already know we're doomed to national insolvency, but let's pin down the underlying--and rarely mentioned--cause. It's the war. right? Well, sort of, but the war could be wound down in a relatively short period of time. Then much of that expense drops off the ledger. Then it's the runaway Pentagon spending, isn't it? Well, that certainly doesn't help, but again, a new president and a change of priorities could reduce that budget, which is discretionary. Actually, it's the entitlement spending which rises inexorably, and which is eating up an ever-larger share of Federal budget: United States Federal Budget:
Mandatory spending accounted for 53% of total federal outlays in FY2007, with net interest payments accounting for an additional 8.6%. Discretionary outlays, which rely on annual appropriations for funding, accounted for 38.2% of total federal outlays in FY2007.
Bush Seeks Budget of $3.1 Trillion: (NY Times)
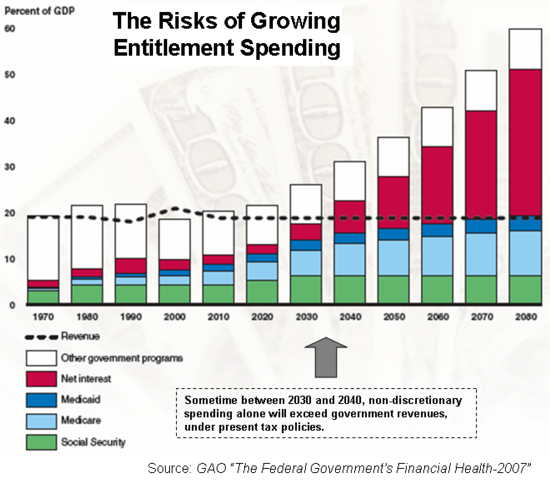
The Pentagons proposed budget, for instance, is $515.4 billion, an increase of 7.5 percent over this year, meaning that military spending would be the highest in inflation-adjusted terms since World War II.The reality is that the cause of our pending insolvency is entitlements, specifically medical/healthcare entitlements. In a nutshell, here's how you drive a government (city, county, state, agency, nation) into insolvency: take a long-term growth rate of 2% per annum rise in revenue and GDP and then mix in a large expense which grows by 6% or more each and every year, year after year. What happens is you end up with a chart like the one below:
Note that Medicare costs have nearly doubled since 1997. Every few years, an estimate of slower growth is issued, a few tweaks are made (see below) to pare a few billion here and there, and a few years later it turns out the programs grew faster than expected. If military spending is restrained to the same rate as GDP for a few years, Medicare/Medicaid will soon far exceed Pentagon spending. Under the most implausibly optimistic estimates issued by the Bush White House, Medicare spending will "only" be $553 billion in fiscal year 2013--a number that is based on cuts which are politically DOA (dead on arrival). Bottom line: Medicare costs will still be rising 2 to 3 times faster than underlying GDP or tax revenues. The more realistic estimate is $600+ billion per year, and we won't have to wait for 2013 to reach that, either. Here is an analysis of President Bush's proposed Medicare cuts and budget: MEDICARE AND THE PRESIDENTS FISCAL YEAR 2009 BUDGET PROPOSAL (source: Henry J. Kaiser Family Foundation)
Medicare is the nations health insurance program for people age 65 and older and people under age 65 with permanent disabilities. The program, which currently covers 44 million people, helps to pay for many important health care services, including physician visits, hospitalizations, and prescription drugs. Medicare spending is expected to be about $420 billion in Fiscal Year 2009, or 14% of federal spending, rising to $553 billion in 2013, or 16% of the federal budget.So how do we rein in unsustainable, inevitably bankrupting medical/healthcare entitlements? Maybe the first step is to identify the underlying causes. The first one, of course, is demographics. The programs were established in the 1960s when the number of workers was vastly greater than the number of benficiaries. But with the Baby Boom about to enter the Medicare system, the ratio of workers to beneficiaries turned impossibly negative. Adding additional pressure is the rising number of very elderly; the number of people living past the age of 80 is skyrocketing. The actuarial basis of Medicare has completely changed, but the program chugs on as if it's still 1969. The second is, of course, that much more can be done medically now. Expensive MRI and tomography tests can be done, horrendously expensive medications can be prescribed, and amazing new surgeries can be done, even on the very elderly (85+ years of age). The third reason is the one nobody talks about: the health of the nation's citizenry has deteriorated due to unhealthy diets and lifestyles. What I am referring to are chronic, largely preventable diseases such as diabetes, which now afflicts an astounding 20 million Americans, diseases which can be traced to obesity and inactivity. I am referring to chronic illnesses that require constant monitoring, medications, testing, etc. for years or decades, not diseases like pneumonia which can be beaten off or cured, after which the patient goes back to a life without constant intervention/care. I am referring to the many chronic conditions which are "side-effects" of a poor diet, smoking, alcohol abuse and lack of exercise. The fourth reason is cultural: death is viewed in the U.S. as either a potential liability or an avoidable error. Death is generally viewed as "preventable," and therefore the medical caregivers have major incentives to err on the side of caution: give the ill person every possible test, bill Medicare, and you can't go wrong. Withhold a test, and it's time to line up the attorneys to fight the malpractice suit. Ironically, mistakes in care seem to be rising along with all the tests and litigation-inspired scrutiny. The fifth reason is that, magically, an endless source of money will attract invoices. It seems medical care in the U.S. is influenced either by cost (if nobody's paying) or litigation avoidance (give every test, prescribe lots of meds, perform surgeries, do something and then bill for it). When anything is "free," it is squandered. That is human nature. It is also human nature to create billings which will pay one's overhead and salary. And if one is a surgeon, it is human nature to see some benefit in an operation, even if the odds aren't favorable. Hope--even the costliest, riskiest kind--springs eternal. Within the circle of elderly I have known personally, a high percentage of the males have died either on the operating table or shortly thereafter. In every case, the surgery was elective; it was not to remove a tumor or clearly identifiable problem, but some "fix" attempted on less well-defined disorders. So what is the solution to a problem with roots in demographics, medical technology, culture and financial "choice architecture"? Many well-intentioned citizens believe that a single-payer "national healthcare" system would reduce administrative costs and therefore lower the cost of providing care. While I am sympathetic to the concept that eliminating paperwork will save some money, I suspect all we'll have is a $1.5 trillion dollar system driving the nation into insolvency rather than a mere $1 trillion system doing so. You can't tax workers $1,000 per year and then spend $250,000 to $500,000 on every senior's last few weeks of life when there's only 3 workers for every retiree. Even the European national healthcare plans which are touted as potential models (France, for instance) are heading for insolvency as the Baby Boom enters high-cost old age. Although I cannot locate any statistics on this, anecdotal evidence suggests that national healthcare plans in Canada, the U.K. and France operate under subtly different assumptions about what care will be provided in extreme old age. Here in the U.S., even very old, very frail people are given very costly surgeries--and as noted above, the result of this stressful, and rather obviously questionable, intervention/"fix" is often death. Nonetheless, the operation's cost--often tens of thousands of dollars, plus thousands more for a few days in the hospital--is billed to Medicare. Do readers in Canada, the U.K. or France have any direct experience of similar care being given the very elderly? Do 89-year olds routinely get new hips and heart surgery in your country? What guides the caregiver in making these kinds of decisions? Are there solutions which will satisfy everyone? Heck no. If we're honest with ourselves and the fact that there simply isn't enough money on the planet to spend hundreds of thousands of dollars on each seniors' medical care when the number of seniors will soon double from 35 million to 70 million, then solutions come in only a few flavors: 1. Ration the costliest, riskiest care. Brain surgery, etc., might be reserved for people under 65. Not a popular idea but this is one way to limit costs to actual revenues/funds available for medical care. To many this seems "UnAmerican" because Americans don't like any limits; everything should be possible. Alas, it isn't when it comes to tax revenues. 2. Place some responsibility on citizens for their own health. We should recall that Medicare isn't "insurance;" we all get ill and die, and that is not at all like the odds of a house burning down. The model for citizens being responsible for their own risk factors is auto insurance; if you are an irresponsible driver, then your insurance costs will skyrocket or you will be unable to obtain insurance. The choice was yours, the consequences are yours, too. If a citizen smoked and has a BMI of 30+ and as a result suffers from heart disease, lung cancer, diabetes and blown-out knees, then we might ask: why shouldn't they pay more than citizens who acted more responsibly? Like a driver who wrecks car after car, maybe we should not be held responsible for "fixing" what they have destroyed. Perhaps these citizens could be offered pain management meds; the rest of their care is up to them. Again, let's recall that wishful thinking has no place here; the system as it is now will founder in a few years. If a long, deep recession is in the offing, then Medicare's financial insolvency is not some distant event--it's very close at hand. 3. Change the "choice architecture" to put more resources into prevention and less into costly "fixes" which often don't even work. Right now, it's practically "free" to prescribe and take costly meds which conflict with each other, and "free" to "try" an iffy surgery in the hopes it actually helps the patient rather than kills them; there is no financial incentive for either provider or patient to emphasize prevention. 4. Connect the dots between an environment built for the convenience of autos/drivers and an illness-producing packaged-food industry with Americans' wretched diets and lack of exercise. Who wants to walk across 6 lanes of asphalt and walk down a grubby, hot barren sidewalk (or in the suburbs, the street, since sidewalks have been dispensed with)? Who can enjoy a bike ride alongside a freeway or equivalent roadway, where death is everpresent? "The Market" fails here, utterly, completely, inalterably; the "free market" True Believer insists that if people want to eat garbage food loaded with salt, sugar and fat, then it's their right to do so, or to choose healthier (immensely less profitable) fresh fruits and vegetables. Nice, but society/taxpayers are then saddled with fixing all the consequences of others' horribly unhealthy diet and lifestyle. You can't have it both ways, free market believers; if "consumer choice" is king and no government interference is needed, then there shouldn't be any government "intervention" in healthcare, either. Abolish Medicare and let the cash-paying consumer set the market. If we taxpayers are being saddled with the costs of unhealthy, heavily-advertised food and an environment which is not conducive to enjoyable exercise and getting to places you want to go on foot or bicycle, then we should also have a say over those causal conditions. 5. Let globalization work its cost-cutting magic on every aspect of medical care in the U.S. We are already seeing people flying to India or Thailand for operations which cost 10-20% of the price in the U.S., and many Americans are having dental work and other care done in Mexico for a fraction of the cost in the U.S. (If oil goes to $300/barrel, we can anticipate Indian and Thai-operated clinics in Mexico.) This alternative is not welcome news to the bloated, inefficient medical system in the U.S., but steelworkers and many others who used to work in industries which vanished under global wage and cost arbitrage can attest that life goes on--just not as lucratively. If we really can't bear to invest some energy in becoming healthier, and we really can't bear to place some limits on very costly care, and we really can't bear to insist that citizens take some responsibility for "lifestyle" illnesses and conditions, then about the only alternatives are either let the system go insolvent and nobody gets any government-funded care, or allow globalization to strip away about $300 billion of the $550 billion annual bill. Yes, you won't have the same legal rights to sue in Mexico or India or Thailand, but again, the choice to do nothing but tweak the dials here and there is a choice for national bankruptcy. Nobody in 2020 is going to get the care being lavished on the current crop of Medicare/Medicaid recipients because the money will have run out. All those who want to pay 50%-60% of their income in Federal taxes to fully fund Medicare into the future, please stand up. I thought so. We don't want to pay the taxes necessary to actually fund Medicare in its current incarnation, but we all want the benefits. Maybe it's time to finally grow up as a nation and accept that expenditures have to match revenues, and choices have to be made; we can't just borrow $40 trillion from the oil-exporting states and China and leave our kids to pay the interest.
We might even wake up one fine morning and discover nobody can loan us the $40
trillion anyway, no matter how much we beg and cajole. Then the hard
choices will have to be made, whether we're in the mood to deal with reality or not.
Why donate to this site? Many blogs are what's been described as "Look!" blogs--basically lists of links from the major media ("Look!") with a bit of comment added. Here at OTM we try to provide original content and fresh analysis. OK, so sometimes we blow it, but then smart readers correct us and you get to read more great commentary. Your financial support, commentaries and readership are the essential elements which keep this dorry afloat. NOTE: contributions are acknowledged in the order received. Your name and email remain confidential and will not be given to any other individual, company or agency.
Thank you, Cheryl A. ($25), for your unexpected and very generous donation
via mail of the book The Great Wave by David Hackett Fischer.
I am greatly honored by your support and readership.
For more on this subject and a wide array of other topics, please visit my weblog. All content, HTML coding, format design, design elements and images copyright © 2008 Charles Hugh Smith, All rights reserved in all media, unless otherwise credited or noted. I would be honored if you linked this wEssay to your site, or printed a copy for your own use. |
| consulting | blog fiction/novels articles my hidden history books/films what's for dinner | home email me | ||